Our poor little boy |
|
|
Will's story horrifies and saddens all who hear it. Friends and family know the story well, as do those brave enough to broach such a difficult topic with us. It is still emotionally draining to explain what happened, let alone how it could happen. (For those reading this outside of New Zealand, please be aware that we are a very developed country and our health system is generally first class. Another thing to note is that we have collectively given up the right to sue for negligence.)
Before all of this, the last time I actually cried was way back in middle school (Year 7) - when one of the Ritalin twins pushed me over in the playground. Usually I can't make it through Will's story without my eyes welling up, but here our story can be told clearly and in considerable detail. For my psychological health, it is important that the story can be told here and in depth, because once the Health and Disability Commissioner's report into Will's treatment is released we have been told to expect considerable media interest. With considerable media interest, comes considerable public interest and there's no way I'm up to telling this story a hundred times over to passing acquaintances and well-meaning strangers in the supermarket. I'm not just scared that it will be emotionally exhausting, I'm afraid that with each telling the raw emotion associated with Will and the events themselves will become habituated and somewhat diminished. That sadness and anger is something I need to hold on to for now. Here I tell Will's story from my perspective, and finish with documents related to the complaints we've made about his lack of treatment. These documents, especially the Health and Disability Commissioner's findings and report outline the negligence of Wellington Hospital across two fateful days. |

Will is admitted back onto the children's ward often
What is meningitis? |
Wednesday 16th October
- Will had a fever in the morning and we took him to our local Medical Center after I finished work where they checked him over and wanted to take a urine sample to test for a bladder infection, which we couldn’t get in time before they closed so they advised us to collect the sample and take it to the After Hours Medical Center.
- The urine sample was duly collected and we took the sample and Will to the After Hours Medical Center. Here, while the doctor was poking and prodding his stomach he vomited. The urine test came back positive for bacteria in his urine (which would later prove contaminated; i.e., bacteria from his skin, the doctors hands, etc.).
- The doctor then advised us to take Will to the Emergency Department at the hospital and this, we duly did.
- At Wellington Hospital, the emergency doctor who checked Will over on his arrival called in the pediatric consultant who was on call.
- The pediatric consultant checked Will over. Took a ‘clean’ urinary sample, which is a sample taken away from contact with the body (i.e. they inserted a catheter). This was negative ruling out the bladder infection.
- When she was examining Will the pediatrician did mention “meningitis” as she thought aloud to herself, but obviously dismissed it as a consideration. She also gave considerable thought as to whether Will should be admitted overnight for further observation, and she almost did admit him, to the point where I was asking my wife what she wanted packed in the overnight bag that I would need to return home for.
- No blood test was performed.
- We were all sent home with instructions to bring him in the next day if he still had his fever, and/or if anything worsened overnight.
- No diagnosis was made or suggested.
Thursday 17th October
- Will was still feverish and had also vomited three or four times during the day. I finished work and we returned to our Medical Center. The doctor there didn’t know what was wrong with him, but could see that he was very sick and had deteriorated since his last visit. He asked us to take him back to the Emergency Department at the hospital. The GP we saw said that he would consult with a pediatrician at the hospital.
- We arrived at the hospital and were taken pretty much straight away to the Children’s ward. Here the doctor (a different one to the one we saw the night before, and very junior, and with minimal pediatric experience) examined Will, took another ‘clean’ urine sample which again proved negative. Why so much focus on a bladder infection which had been ruled out the previous day?
- She diagnosed Will as having a gastro-intestinal bug. Now, neither of our kids has had a gastro bug before, but from other parents this didn’t sound right to me – none of the diarrhea or vomiting stories we’d heard about. When I questioned this diagnosis (a gastro bug without diarrhea), she reasoned me through it outlining why she felt that this was the correct diagnosis, which I accepted.
- She also left us to consult with someone over the phone. I wish this this had set some alarm bells ringing. I didn't know just how junior this doctor was at the time. It turns out she was a second year intern at the hospital. This means that she was being rotated through different wards every three or so months to gain experience. At this point in time, this was the 'doctor' making life and death assessments for all children in New Zealand's capital city.
- I asked about a blood test, and she dismissed this as being unnecessary because it would be uninformative. A blood test would have picked up meningitis, especially bacterial meningitis.
- This doctor seemed very hesitant about getting samples. She made us wait hours to try and get a clean urine sample, and when we got fed up, she faffed about trying to get the catheter in and the nurse take over in the end. Was she similarly hesitant about drawing a blood sample from William because in babies this is not the easiest thing to do?
- She also said, with certainty, that with this gastro bug his fever was likely to continue for up to five days. She made the diagnosis, gave us a sugar and salt drink for dehydration and made no suggestion to return if things continued, or indeed, worsened (unlike the pediatrician the previous night).
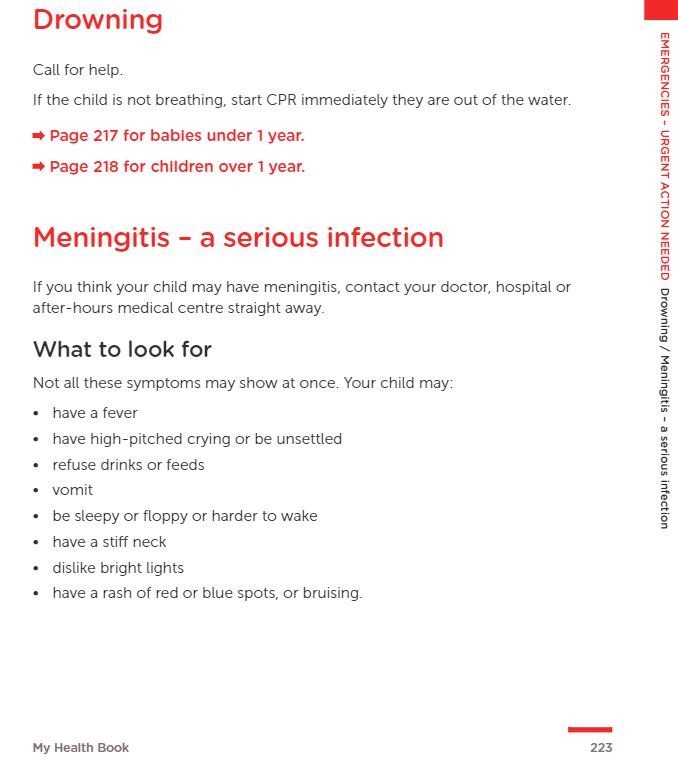
Meningitis symptoms listed in the book handed out to every parent and with every child in New Zealand
|

A link to the My Health Book where parents are expected to know the symptoms of meningitis, but not pediatric doctors?
|
Friday 18th - Monday 21st October
- Will was feverish for the next three days (Friday - Sunday) without vomiting. He didn’t sleep Sunday night.
- On Monday morning Will was still sick and feverish so Wendy took him back to the emergency department, where they did a lumbar puncture, diagnosed meningitis but could not then prevent him from going into seizures.
- If they had have diagnosed meningitis, or kept him in for observation, or not have misdiagnosed him, or even simply not have made a diagnosis (we would have bought him in again the next day) then Will’s outcome would have been far, far different to the terrible prognosis he now has. Time is of the essence in meningitis.
- Meningitis is one of the diseases of childhood that is given its own section in the ‘My Health Book’ (see above) that is given to all parents in New Zealand. William’s symptoms on the 16th and 17th of October match those listed in this book. It is very difficult to accept, on two occasions, that the 'pediatric specialists' responsible for assessing sick children presenting to the children’s ward of the main hospital in New Zealand's capital city did not pick up on these symptoms, or ask the right diagnostic questions to elicit those symptoms. Meningitis must be basic medical knowledge that any children’s doctor needs to know and be aware of. And, these doctors must err on the side of caution and do tests.
Starship Children's Hospital - Late October to late November
- The slow unfolding of a parent’s worst nightmare ... This next phase is more difficult to remember and recount. Emotions cloud everything and sleep deprivation wreaks havoc with memory as days and nights blur into a disjointed and jumbled month.
- I’m in the middle of a Monday, the school week has just started. I receive a call from my wife that she was at the hospital and things were serious with Will, but she doesn’t know what is wrong yet. While I’m arranging cover for my afternoon classes, with our assistant principal looking at me slightly dubiously and wondering if this is me trying to skive off to an afternoon of unfettered freedom (it’s in her job description to be suspicious of teacher motives, but she’s lovely, warm and caring). Another phone call. This time it’s the hospital saying I need to come down to Ward 1 now, and still not saying what is wrong.
- Ten minutes later I’m at the hospital, I walk into the Children’s Ward and come face to face with the young intern who sent us home with the gastrointestinal diagnosis, she’s walking towards me. I don’t stop walking as I ask what’s wrong. She says hesitantly “meningitis”. Immediately an ice cold dagger enters my heart, I know what meningitis is and I know it’s very bad. The implications hit me immediately, it’s been far too long – today’s Monday and we had Will here last Wednesday. Fuck. Fuck! I walk faster towards a small crowded room of busy, slightly nervous doctors and nurses. My beautiful, fragile boy’s on a small cot with lines in his veins, electrodes dotting his skin and head and connected to machines. I would become expert in these machines over time. All I know now are that things are beeping that shouldn’t be beeping. My wife is seated, crying and inconsolable. A nurse asks me hopefully if I’m the father – a rational, level-headed person to calm my wife and provide further information. Tears start running down my face. My first tears in twenty odd years.
- Will’s quickly shuttled to the intensive care unit (ICU) and the doctors and nurses are professional and reassuring. More machines. The hospital beds here are adult-sized and Will looks ridiculously out of place, incongruous beauty connected to stark technology. Starship Children’s Hospital is mentioned. Their doctors are flying to us now. More reassurance. The best children’s doctors in the country are coming for us to take us to New Zealand’s specialist children’s hospital.
- Doctor after doctor tries to get a good line into a decent vein (artery?) that is robust enough to maintain an intravenous line for weeks. No one can. The flight doctor and nurse arrive in a blue blur of overalls, just one more thing out of kilter in this universe now tilted slightly off-axis. He too tries for the line and fails. This is hard to take, these needles are large, and I’ve never been particularly needle friendly. A decision is made to put Will under a general anaesthetic, perform an operation to get the line in before he’s moved to Starship. Eventually we see him again, his neck is bandaged and the new line is embedded in his neck – this meningitis has gone for the jugular.
- It is now early morning and the streets of Wellington are quiet as the ambulance makes its way to the airport. No flashing lights or sirens, no sense of urgency and almost a sense of calm. The Life Flight plane is small and we are forced to sit away from Will. He lies at the rear of the plane with his doctor and nurse.
- On landing the doctor asks if this is Will’s first time on a plane. He gives us a stuffed toy plane – a cutesy version of the Life Flight craft. Another ambulance waits for us. It’s still early and Auckland’s traffic has yet to build. Starship. PICU (Paediatric Intensive Care Unit). We are introduced to doctors, nurses and administrators but names go over our head. We have a single nurse devoted to watching him and she doesn’t take her eyes off him. She’s very professional. We are shown to our accommodation in the same building. It’s a tiny windowless cell. We talk, hold each other and cry. We’re both in shock. We wind our way down to PICU and wait.
- Things begin to pick up in the morning. Nurses change over, more doctors, more bustle. We make difficult calls to family. My poor father, he can sense my distress, the degree of panic in my conversation with him. I can’t talk to anyone without crying and because I haven’t cried in twenty years, I really don’t know how to deal with this at all. I ask him to inform the family. He doesn’t quite get it unfortunately. Twenty minutes later I take a call from my sister. After figuring out that it is unlikely that we would be in Starship for hepatitis, as my father’s been telling people, she’s already guessed it is meningitis. Hepatitis, god I wish. My father or sister have to repeat their phone calls to family.
- We meet with neurologists and infectious disease specialists. A neurosurgeon is introduced. I actually understand a lot of what they’re talking about. I have two degrees in Psychology and have studied neuropsychology and physiological psychology so I ask them to not dumb-down any information they provide. What I don’t know much about at this stage is meningitis. Google lets me know that there are different types of meningitis. Will has bacterial meningitis which Google informs us has the worst prognosis. Everyone is still very reassuring, telling us that his chances are good. Will is taken away for a scan. His head is bulging as the bacterial infection rages, the inflammation swells brain tissue and pus begins to build up. The decision to operate to relieve cranial pressure is made.
- He’s gone a long time and comes back with a head bandage to match the ones on his neck, hands and feet. Two holes have been drilled and pus has been ‘washed’ out. When the bandages are changed, we see the scars of this surgery and are somewhat taken aback. Where we’d perhaps been expecting nice little drill marks, we see that flaps of skin have been pulled back to give the surgeon access to his skull. He looks terrible, but people are still reassuring.
- He wakes up! He drinks my wife’s milk! Everything’s going to be fine, surely? Our doctors are pleased and, in hindsight, look somewhat surprised. It’s a good day or two as we take turns cuddling our son and he continues to feed.
- First he stops feeding, then he stops breathing. He’s placed on a ventilator. His brain is self-destructing in a slow controlled process called apoptosis, or programmed cell death. Oversimplifying things, healthy brain cells surrounding infected and inflamed cells are killing themselves in an effort to stop the disease progressing further, and there is nothing doctors can do about it.
- Time passes and Will wakes up and stabilises. He’s taken off the ventilator and this time my wife can’t get him to feed, which distresses her more than most other things occurring at this time. His seizures start and an EEG machine is brought into monitor his brain activity.
- He progresses out of PICU and into HDU (High Dependency Unit). From here new tests provide a better idea of his prognosis. Scans show the extent of his brain damage, and it’s bad but not critical. Doctors talk about cerebral palsy. We research cerebral palsy and find stories and videos of the most delightful kids and their families. It’s certainly not what we had hoped for our son, but it looks manageable. Maybe he’ll need assistance in walking, maybe he’ll need a wheelchair. He will be able to communicate with us, even if the parts of his brain that control motor function won’t form speech quite so clearly. Breaking Bad has just finished here, and Walter White’s son (Junior) forms much of the schema I develop for cerebral palsy, and he’s cool.
- Over time, tubes and lines are steadily removed leaving him with just the nasogastric tube (NGT; food, liquid and medicines) and his IV line (antibiotics). Our son doesn’t really move which is concerning to us, no little arms and legs kicking. He looks like a little glow bug – a head with a body wrapped in a tapering sheet, glowing red at the bottom with light from a monitoring device. We haven't seen him smile yet. Doctors are still reassuring.


Will's private jet to Starship Children's Hospital
|


Starship Children's Hospital - Auckland
|
Wellington Children's Ward - Late November to late January
- The Life Flight returns us to Wellington, and we arrive back in the Children’s Ward where it all started.
- I return back to teaching. The school year is just about done and my senior school students have already left for exams. Things seem different here and most people tip toe around me.
- Someone has to stay with Will, and my wife and her mother take turns. When school holidays start, I join this roster. We see the Wednesday 16th paediatrician a few times. It’s awkward and she expresses her regret and offers apologies. We don’t see the young intern again until she appears in the dead of night to ask my wife a few questions, it is odd, cagey and awkward. We suspect she shouldn’t have been there. She doesn’t offer an apology or ask how Will or the family is. We never see her again.
- William’s seizures increase, and new medications are tried. He becomes increasingly unsettled and cries loudly and often, morphine settles him. We are called into another family conference. Lots of people are here this time. We are told Will’s last scan shows that he has lost all of his cerebral cortex, apart from a section towards the back of his brain and that his prognosis is bleak. Each time we have one of these conferences, the news always gets worse, but no one has prepared to us for anything like this. There is no reassurance from our doctors any more. Our head paediatrician seems somewhat shocked at the extent of the brain damage. Will won’t have control of his arms and legs, be able to control and support his head on his own, he won’t even have enough muscle control to be able to swallow. He will likely be blind and deaf. We are asked to consider various intervention options as they are needed in the future. We are appalled that one of the options tabled include the removal of our son’s feeding tube and letting nature run its course. Naturally, we come out of this meeting shattered.
- Through trial and error, changing medicines and doses, the doctors are finally able to get Will to settle and we can look at bringing him home.
Reports and documents about Will's initial treatment at Wellington Hospital
Apology from Wellington Hospital
|
|

|